

Authors Dr. Sher Mohamamd and others discuss Transjugular Intrahepatic Portosystemic Shunt (TIPSS) and its role in the management of portal hypertension.
The history of TIPSS
Transjugular Intrahepatic PortoSystemic Shunt (TIPSS) was first described by Josef Rosch in 1969. He was a visiting professor at the University of California, where he performed the first TIPPS after making an accidental entry into one of the branches of portal vein while attempting diagnostic trans-jugular cholangiogram on animals. [1]. Research was carried on as to how to maintain the shunts by experimenting with Teflon tubes and silicone covered spring coils; the primary challenge was how to maintain the patency of the shunt and how to prevent shunt from becoming thrombosed [1].
In 1982, Dr. Ronald Colapinto at the University of Toronto was the first to attempt human balloon dilated TIPSS but was unsuccessful until 1985, when self-expanding bare endovascular stents were introduced [2]. In 1988, the first successful TIPSS was realised by M. Rossle, G.M. Richter, G. Noldge and J. Palmaz at the University of Freidburg.
The role of TIPSS in the management of portal hypertension has been established since 2005. Since 2009, Budd-Chiari syndrome has been added to the list of indications for TIPSS [2]. Currently, TIPSS is the preferred procedure for the treatment of portal hypertension that is refractory to medical therapy, replacing the surgical portacaval shunt in that role.
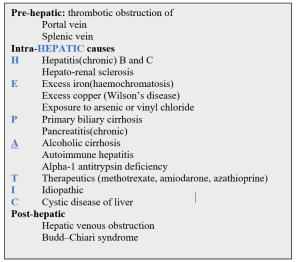
Causes of portal hypertension
Liver cirrhosis may lead to the development of portal hypertension, which has a significant impact on patient outcomes and survival. These patients are clinically challenging and costly to manage, often requiring treatment for consequences of liver failure such as ascites, variceal haemorrhage, sepsis, and renal failure. The principal causes of portal hypertension are briefly outlined in table-1.
Table-1
TIPSS insertion offers a minimally invasive option for lowering raised portal pressure, which can provide symptomatic relief and confer a survival benefit in selected patients suffering the complications of portal hypertension.
Since the mid-1980s, success rates have increased as endovascular and radiological technologies have improved.
Indications for TIPSS
Significant evidence [4.5]
- Refractory ascites
- Variceal bleeding
Limited evidence [4,5]
- Portal hypertensive gastropathy
- Refractory hepatic hydrothorax
- Hepatorenal syndrome
- Hepatic veno-occlusive disease
- Budd–Chiari syndrome
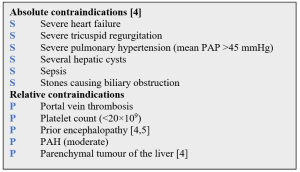
Contraindications to TIPSS are outlined in table-2
Table-2
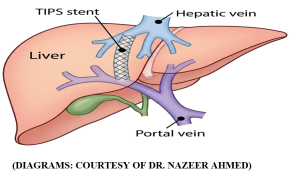
What is achieved with TIPSS procedure
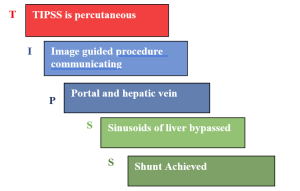
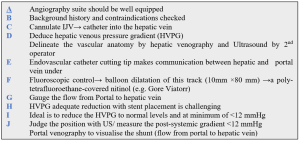
Table-3: Steps in doing TIPSS procedure are outlined
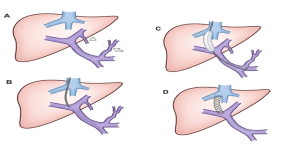
Arrowhead (umbilical vein) and arrow (left gastric vein)
Risks and complications of TIPSS
In the hands of an experienced radiologist, the operative mortality is less than 1%.
Table-4: 5Ts outline the threatening complications of TIPSS
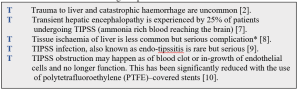
*A less common, but more serious complication, is hepatic ischemia causing acute liver failure. While healthy livers are predominantly oxygenated by portal blood supply, long-standing portal hypertension results in compensatory hypertrophy of and increased reliance on the hepatic artery for oxygenation. Thus, in people with advanced liver disease the shunting of portal blood away from hepatocytes is usually well tolerated. However, in some cases suddenly shunting portal blood flow away from the liver may result in acute liver failure secondary to hepatic ischemia.[8]
Problems associated with Angio/Radiology Suite
A Angio suite is a remote location from theatres
B Back up/help lacking
C Cold environment, body warmer may hinder radiologist’s task.
D Direct access to patient limited
E Exposure to radiation/lead cover needed for long time
Problems with Patients presenting for TIPSS
A Ascites causing hydrothorax
B Breathing difficulty when supine (needed for TIPSS)
C Coagulopathy/thrombocytopaenia [11]
D Delayed recovery after GA expected
E Encephalopathy→ can become worsened post-TIPSS
F Full stomach due to ascites→ RSI needed
General anaesthesia is recommended by many as the preferred technique on the grounds of safety, particularly when complications occur. This requires the appropriate equipment, monitoring, and assistance as mandated by the AAGBI.
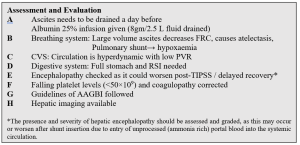
Table-5: Pre-op Assessment
Anaesthetic management of TIPSS
Insertion of TIPSS is a relatively long procedure lasting 2-3 hours in a location away from main theatres. Although intravenous sedation using dexmedetomidine has been used successfully by some clinicians, general endotracheal anaesthesia is generally the preferred option, albeit there is risk of complication from anaesthetic drugs.
General anaesthesia in an angio suite provides optimal patient comfort and pain relief, airway control and haemodynamic manipulation by anaesthetist, leaving the radiologist free to concentrate fully on technical aspects of the procedure. The technical aspects of anaesthetic management are outlined in table-6.
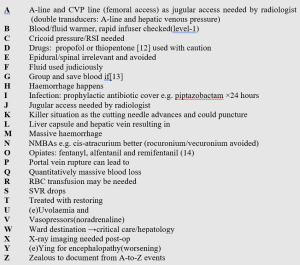
Table-6: Succinct Summary of Anaesthetic Management of TIPSS: Interventional Radiology Suite
Post -operative Problems
H Hepatic encephalopathy
H Hepatic infarction
H Haemorrhage
H Haemodilution and electrolyte imbalance
Patients are managed either on critical care, hepatology, or gastroenterology wards and are subject to early warning scoring and frequent medical review. Given the potential for multisystem decompensation, access to critical care outreach and high dependency care in the post-procedure period is necessary. However, given the nature of the underlying disease and often guarded prognosis, escalation of care must be carefully considered with appropriate ceilings of care set in a multidisciplinary environment, ideally in advance of any intervention.
Post-TIPSS Metabolism of Drugs
The pharmacokinetics changes after TIPSS:
The ‘first-pass’ is bypassed, oral drugs which are absorbed from the gut into the portal vein and flowing via TIPSS, are not metabolised in the liver and reach the systemic circulation. That means a much higher concentration of drug will be available at the receptor sites.
Decrease hepatic clearance: Even with IV administered drugs, blood flow is shunted away from metabolising enzymes (CYP450 pathways) inside the liver, drastically decreasing the drug elimination.
Because of TIPSS, standard doses of many medications can suddenly become toxic. Clinicians need to adjust doses carefully:
- Statins: the bioavailability of atorvastatin and rosuvastatin can be significantly increased to toxic levels causing rhabdomyolysis.
- Cardiac drugs e.g. propranolol, bisoprolol and nifedipine (bioavailability increased)
- Anticonvulsants e.g. phenytoin needs close monitoring
- Sedatives e.g. midazolam will have prolonged effect
- Antiretroviral e.g. dolutegravir metabolism is affected
- Steroids e.g. budesonide metabolism is impacted.
Future of TIPSS
The current day TIPSS technique has evolved from an accidental communication between hepatic and portal veins and has seen many developments and improvements but two problems still exist i.e. Shunt blockage and hepatic encephalopathy.
The PTFE-covered stents have shown promising results as regards the shunt patency but problem still happen with the patency of TIPSS.
The problem with encephalopathy is likely to be there for the years to come. Individual patient’s factors include overall patient health, patient compliance with taking medicine and dietary variations. The ideal next step will be in TIPSS design i.e. variable diameter TIPSS that can change the degree of shunting to accommodate for varying requirements. For example, if encephalopathy happens, the TIPSS can be temporarily narrowed (with help of artificial sphincter) to decrease the flow across the shunt. Electromagnetic doorways or apertures are aspects the biomedical engineering could look at.
The introduction of small calibre (<8 mm) TIPSS is a promising approach to reduce shunt-related complications. Its feasibility with the new controlled expansion endoprosthesis (GORE® VIATORR® CX 8-10 mm) has not yet been explored [15].
Conflict of Interest: None Declared
Authors and Contributors:
Dr. Sher Mohamamd1, Dr. Parhaizgar Khan2, Dr. Mujahid Ul Islam3, Dr. Sibghat Ullah Khan4, Dr. Nazeer Ahmed5, Dr. Muhammad Ahmad Saroosh Saleem6, Dr.Ayesha Shafqat7 , Dr. Ahmed Naeem8
1.Consultant Anaesthetist(retired), STH NHS FT Sheffield
2.Professor of Anaesthesia, Khyber Teaching Hospital Peshawar
3.Professor of Anaesthesia, RMI Peshawar
4.Consultant Anaesthetist, Hamad General Hospital, Doha Qatar
5.Consultant Anaesthetist, Hamad General Hospita, Doha Qatar
6.Senior registrar, Anaesthetics, Shalimar Hospital Lahore.
7.Trainee Anaesthetist, Fatima Memorial Hospital, Lahore
8.Trainee Anaesthetist, Saleem Memorial Hospital,Lahore
References
- Ferral, Hector; Lopez-Benitez, Ruben (February 2023). “The History of the Transjugular Intrahepatic Portosystemic Shunt”. Seminars in Interventional Radiology. 40 (1): 19–20. doi:10.1055/s-0043-1764284. ISSN 0739-9529. PMC 10159701. PMID 37152791.
- Saad, Wael E. (September 2014). “The history and future of transjugular intrahepatic portosystemic shunt: food for thought”. Seminars in Interventional Radiology. 31 (3): 258–261. doi:10.1055/s-0034-1382794. ISSN 0739-9529. PMC 4139426. PMID 25177087.
- García-Pagán, Juan Carlos; Caca, Karel; Bureau, Christophe; Laleman, Wim; Appenrodt, Beate; Luca, Angelo; Abraldes, Juan G.; Nevens, Frederik; Vinel, Jean Pierre (June 2010). “Early use of TIPS in patients with cirrhosis and variceal bleeding” (PDF). The New England Journal of Medicine. 362 (25): 2370–2379. doi:10.1056/NEJMoa0910102. hdl:2445/47046. ISSN 1533-4406. PMID 20573925. {{cite journal}}: |last3= has generic name (help)
- Amesur, Nikhil B.; Novelli, Paula (2025), “Transjugular Intrahepatic Portosystemic Shunt”, StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30020640, retrieved 2025-05-07
- Copelan, Alexander; Kapoor, Baljendra; Sands, Mark (September 2014). “Transjugular intrahepatic portosystemic shunt: indications, contraindications, and patient work-up”. Seminars in Interventional Radiology. 31 (3): 235–242. doi:10.1055/s-0034-1382790. ISSN 0739-9529. PMC 4139433. PMID 25177083.
- Zhang, Jian-Bin; Chen, Jie; Zhou, Jin; Wang, Xu-Ming; Chen, Shu; Chu, Jian-Guo; Liu, Peng; Ye, Zhi-Dong (2021-07-06). “Systematic review and meta-analysis of trans-jugular intrahepatic portosystemic shunt for cirrhotic patients with portal vein thrombosis”. World Journal of Clinical Cases. 9 (19): 5179–5190. doi:10.12998/wjcc.v9.i19.5179. ISSN 2307-8960. PMC 8283597. PMID 34307565.
- Rossle M, Piotraschke J. Transjugular intrahepatic portosystemic shunt and hepatic encephalopathy. Dig Dis 1996; 14:12–19.
- Mayan H, Kantor R, Rimon U, Golubev N, Heyman Z, Goshen E, Shalmon B, Weiss P.: “Fatal liver infarction after transjugular intrahepatic portosystemic shunt procedure.” Liver, 2001;21(5):361-4.
- Mizrahi, Meir; Adar, Tomer; Shouval, Daniel; Bloom, Allan I.; Shibolet, Oren (February 2010). “Endotipsitis-persistent infection of transjugular intrahepatic portosystemic shunt: pathogenesis, clinical features and management”. Liver International. 30 (2): 175–183. doi:10.1111/j.1478-3231.2009.02158.x. ISSN 1478-3231. PMID 19929905.
- Rössle, Martin (November 2013). “TIPS: 25 years later”. Journal of Hepatology. 59 (5): 1081–1093. doi:10.1016/j.jhep.2013.06.014. ISSN 1600-0641. PMID 23811307.
- NICEguidelineCG141.Acuteuppergastrointestinalbleeding: management. 2012. NICE. Available from www.nice.org.uk/ guidance/cg141
- VajaR,McNicolL,SisleyI.Anaesthesiafor patientswithliver disease. Contin Educ Anaesth Crit Care Pain 2010; 10:15–9
- DeGasperi A, Corti A, Corso Ret al. Transjugular intrahepatic portosystemic shunt (TIPS): the anaesthesiologist point of view after 150 procedures managed under total intravenous anaesthesia. J Clin Monit Comput 2009; 23: 341–6
- Villanueva C,Colomo A,Bosch Aetal.Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med 2013; 368:11–21
- https://doi.org/10.1016/j.dld.2023.01.109
